
Table of Contents
Intro: Framing Change Risk
The high-stakes transition to Linux in healthcare is not a technical battle—it is a governance challenge. Many IT leaders still treat Linux as a drop-in replacement to cut licensing costs, but its real value is as the foundation of a resilient, clinical-grade operating model. Linux improves healthcare outcomes only when adoption is driven by a risk-led framework that prioritizes clinical uptime, medical device safety certifications, and automated regulatory evidence—not just cost-cutting.
In practice, Linux and open source are often sold on cost and security alone, yet healthcare environments are complex, highly regulated, and safety-critical.
The real competitive and clinical advantage comes from how effectively hospitals manage change risk, not which operating system they choose.
A strategic, risk‑led framework helps decision‑makers assess Linux adoption across clinical, operational, and compliance dimensions.
Watch: Linux in Healthcare, Beyond Cost and Security
Summarizing the key governance, risk, and compliance themes from this article for busy healthcare IT leaders.
Key Takeaways
-
Linux’s value in healthcare comes from governance, not the kernel itself; outcomes depend on how well teams manage clinical risk, change control, and interoperability.
-
Treat Linux adoption as a workload‑by‑workload decision: some systems are Linux‑ready, others must wait for vendor/certification changes, and a few are effectively Linux‑never in today’s regulatory context.
-
Security and compliance gains only appear when Linux is paired with hardening baselines, observability, and structured processes that turn configs and logs into audit‑ready evidence.
-
TCO is multi-dimensional: license savings can be offset by skills, tooling, and governance investments, so leaders should model costs over several years, not just Year 1.
The Myths
Linux is frequently touted as inherently secure and cost-saving. Open source can eliminate licensing fees and vendor lock-in, offering flexibility that proprietary systems may lack. Evidence suggests open-source tooling can reduce infrastructure costs and boost interoperability when integrated well with existing systems.
Why is Linux used in healthcare?

Security is a major reason healthcare organizations adopt Linux. It is widely used in industries that handle sensitive information, and when properly configured and maintained, a Linux-based stack can be hardened against common malware and intrusion attempts. This makes it a strong foundation for enforcing encryption, access controls, and data loss prevention to help protect patients’ data in transit and at rest, often alongside dedicated solutions for securing patient data.
However, simply replacing one OS with another does not automatically deliver security by default, nor does it eliminate the long-term operational costs of governance, integration, and ongoing alignment with healthcare cybersecurity guidance.
Risk-Led Model
A risk-led model assesses Linux adoption not as a binary good/bad choice but as a continuum of clinical, regulatory, and interoperability implications. For example, open-source EHR systems like OpenMRS and OpenEMR are widely deployed in low-resource settings precisely because they reduce upfront licensing costs and offer customization.
At the same time, interoperability with national standards or existing proprietary systems often remains a key constraint, requiring robust governance and data strategy. A Linux Foundation report highlights that open architectures support interoperability but must be paired with organizational processes to succeed.
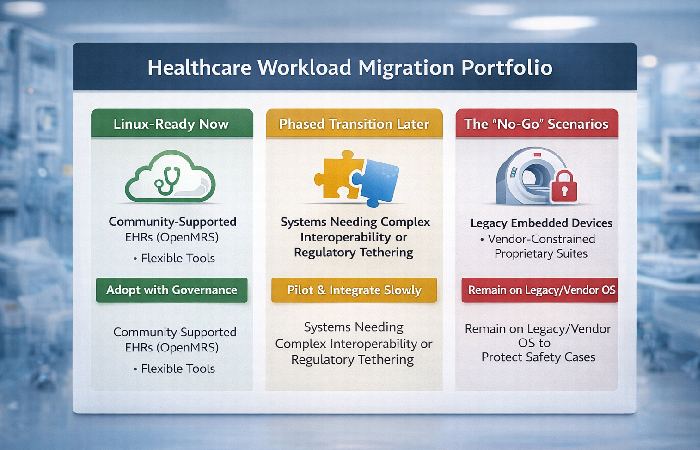
Workload-First Strategy
Not all workloads are equally suited for immediate Linux adoption:
-
Linux-ready: systems like open-source EHRs (OpenMRS, GNU Health) that are community supported and designed for flexibility.
-
Later: systems where interoperability or regulatory tethering requires phased transitions.
-
Never: legacy clinical devices with vendor constraints or proprietary requirements.
This portfolio thinking helps avoid broad platform shifts that can disrupt clinical workflows or introduce disproportionate integration costs.
Failure Patterns
Challenge 1 — Vulnerability Management Paradox
Linux’s open-source model means many contributors rapidly find and fix vulnerabilities, but it also means a high volume of patches for maintainers to track — particularly in embedded medical devices. Recent analysis notes that Linux’s frequent CVE activity complicates regulatory compliance and device certification processes.
Challenge 2 — Security Assumptions
Open source does not guarantee secure implementations. Without mature governance, open-source stacks can be more exposed to risk because organizations lack accountability structures to manage code updates, dependencies, and quality control — a known risk in large OSS ecosystems used across the health sector.
Operating Model
Hospitals and health systems must embed Linux governance within a structured operating model that includes:
-
Change control processes tailored to clinical uptime windows.
-
Configuration baselines aligned with compliance requirements and informed by established Linux security hardening guidance.
-
Patch orchestration that balances immediacy with clinical safety.
Simply shifting OS layers isn’t sufficient — the maturity of governance and SRE practices determines outcomes.
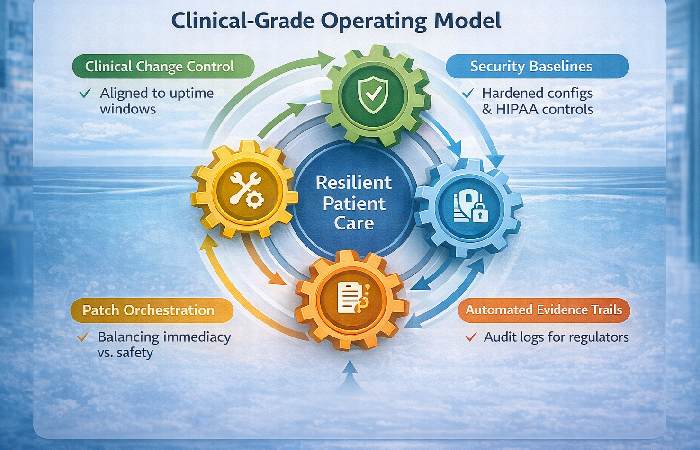
Audit Reality
Regulators (HIPAA, GDPR, etc.) require evidence trails: audit logs, access control documentation, and risk assessments. Linux systems can meet these demands, but organizations must design logging, change tracking, and incident response into their deployments — it doesn’t occur by default. Public examinations of OSS in health info systems emphasize this requirement for structured policies and evidence rather than assumptions about openness equating to compliance.
90-Day Playbook
-
Inventory Workloads: Classify by clinical risk, vendor constraints, and integration complexity.
-
Define Baselines: Create hardened configuration templates tied to regulatory controls.
-
Pilot Projects: Deploy Linux stacks on non-critical systems first, gathering evidence and refining processes.
-
Governance Ramps: Stand up change control boards and SRE teams with healthcare-specific SLAs.
The “No-Go” Scenarios
There are legitimate cases where Linux adoption is not ideal:
-
Systems with tight regulatory certification where vendor support is central.
-
Medical devices whose firmware cannot be modified without breaking safety cases.
-
Highly proprietary clinical suites where migration cost and risk outweigh benefits.
These “No-Go” decisions protect clinical workflows and regulatory standing.
1. Thesis & Big Idea — a clear, original claim grounded in real evidence
Linux and open source can transform healthcare IT — but only when adoption decisions are driven by risk management, interoperability planning, and operational governance, not by simplistic narratives about cost or security alone.
2. Published Evidence & Examples — studies, documented deployments, usage patterns
OpenMRS is a high-impact EHR platform used in over forty countries and designed for low-resource environments, showing how open source can scale in global healthcare when aligned with governance and community support.
OpenEMR, certified under meaningful use criteria and supporting integrated records and billing, illustrates how open-source systems can meet rigorous functional requirements.
Evidence also shows open source boosts interoperability potential, but institutional readiness is a significant factor in success.
3. Documented Failures or Counterintuitive Findings — real challenges or case lessons
Despite the promise, managing Linux in medical embedded systems has exposed vulnerability management complexity that catches many healthcare IT teams off guard — illustrating that open source’s transparency introduces a flood of identified issues that must be operationally managed.
Open-source codebases in healthcare may contain high-risk components if not updated and audited regularly, underscoring the need for disciplined maintenance.
4. Contrarian / Nuanced Insight — push beyond the usual “Linux is cheaper/secure” narratives
Cost savings and security benefits attributed to Linux often overlook the governance, integration, and interoperability overhead required to realize them. Healthcare’s regulatory complexity and clinical safety stakes mean that these benefits accrue only when paired with structured change control and risk assessment.
5. Takeaways & Practical Decision Rules — based on real evidence
-
Assess clinical impact first: Prioritize workloads where Linux’s flexibility aligns with quantifiable improvements.
-
Govern with evidence: Treat compliance and audit readiness as operational fundamentals, not add-ons.
-
Balance pilot and scale: Validate in low-risk areas before broad expansion.
6. Conclusion
Linux is not just an OS — it’s a strategic choice that must be integrated with governance, interoperability, and risk management. For experienced healthcare IT leaders, the real value lies not in bias toward Linux or away from it, but in making decisions grounded in risk, evidence, and clinical impact, and in understanding how broader hospital technology ecosystems support those choices.
FAQs
1. Is Linux inherently more secure for HIPAA environments?
No. Linux offers strong security features, but most breaches come from misconfiguration and weak processes, not the kernel itself.
2. Can Linux be used with FDA-certified medical devices?
Sometimes. If a device is certified as a full stack, changing the OS can affect its safety case, so many such systems are effectively Linux‑never under current contracts.
3. What is the real TCO of moving to Linux?
License costs usually drop, but overall TCO can rise short term as teams hire Linux/SRE talent and invest in automation and observability.
4. How can Linux help with audit compliance?
With Infrastructure as Code and standard baselines, Linux makes it easier to map configs to HIPAA/ISO controls and generate repeatable evidence from code and logs.
Disclosure:
Insights in this article based on internal project experience and publicly available research and are shared for informational purposes only.
They do not constitute legal, regulatory, or clinical advice, and organizations should validate all decisions with their own compliance, legal, and clinical safety experts. Parts of this article were developed with the assistance of AI-based writing tools and then reviewed and edited by human subject‑matter experts.